If you read the dental press, AI in UK dentistry sounds like radiographs and robots. The reality, talking to practice owners every week, is more boring and more profitable.
Six things private dental practices are doing with AI right now. What it looks like in a normal practice. Roughly what it costs. Roughly what it returns in the first 90 days. Where a tool name is essential, it is named. Where it would read as an ad, it is not.
1. Catching the calls the front desk misses
The most adopted use case in 2026 is not clinical. It is the phone.
A practice with a single front-desk seat misses calls every time the manager is in clinic, on lunch, on another call, or away from the desk. private practices typically miss 22% to 45% of inbound calls. Hiya research puts the share of voicemail-listeners who never leave a message at 80%.
What practices are doing: an AI voice receptionist sits on the line behind the manager. When the manager picks up, the AI does nothing. When the manager does not pick up within three rings, the AI answers, identifies the caller's reason, books straight into the practice management system if it is an appointment request, and notifies the manager if it is anything else.
Rough setup: £450 to £900 per month, flat. Two weeks to integrate with Dentally, SOE, R4, or Carestream.
Rough return at 90 days: one new private patient recovered per week pays for the system several times over. Practices we work with typically see net positive cash-on-cash inside the first month.
For the honest comparison against keeping a second receptionist on, see: AI receptionist vs dental practice manager.
2. Bringing lapsed patients back without anyone making calls
Every practice has a list of patients who have not been in for 12, 18, or 24 months. Most of them did not leave for a reason. They drifted.
AI-driven recall now sits on top of Dentally or SOE, scans the patient list for overdue recalls, picks the right channel per patient (SMS for the ones who reply to texts, email for the ones who do not), writes the message in a tone the practice approves once, and runs the sequence.
Rough setup: £180 to £400 per month depending on patient list size.
Rough return at 90 days: 8% to 15% list reactivation. On a 4,000-patient list, that is 320 to 600 patients back through the door without anyone picking up the phone. At an average UK private check-up of £85 and a hygiene visit of £75, the recall cost is recouped in week one of the campaign.
The practices that get the most out of this are the ones with the cleanest patient databases. The practices that get the least are the ones that have not updated their records since 2022. The system surfaces that problem fast.
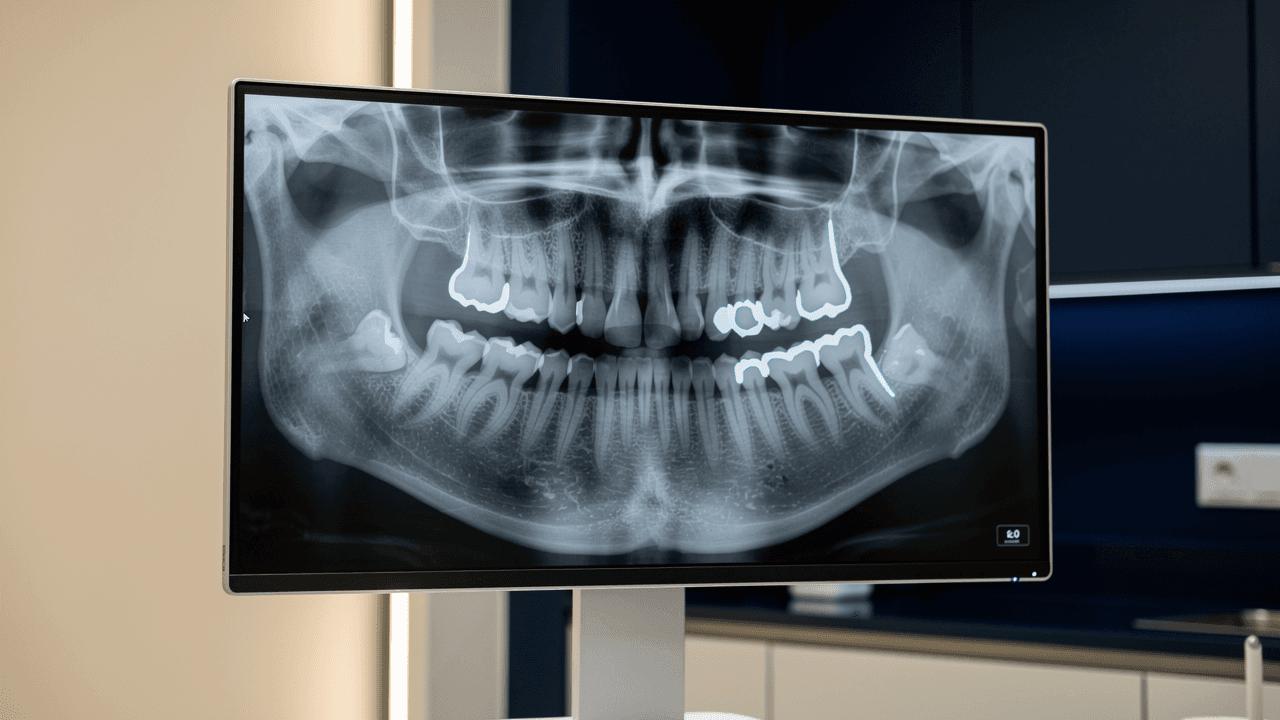
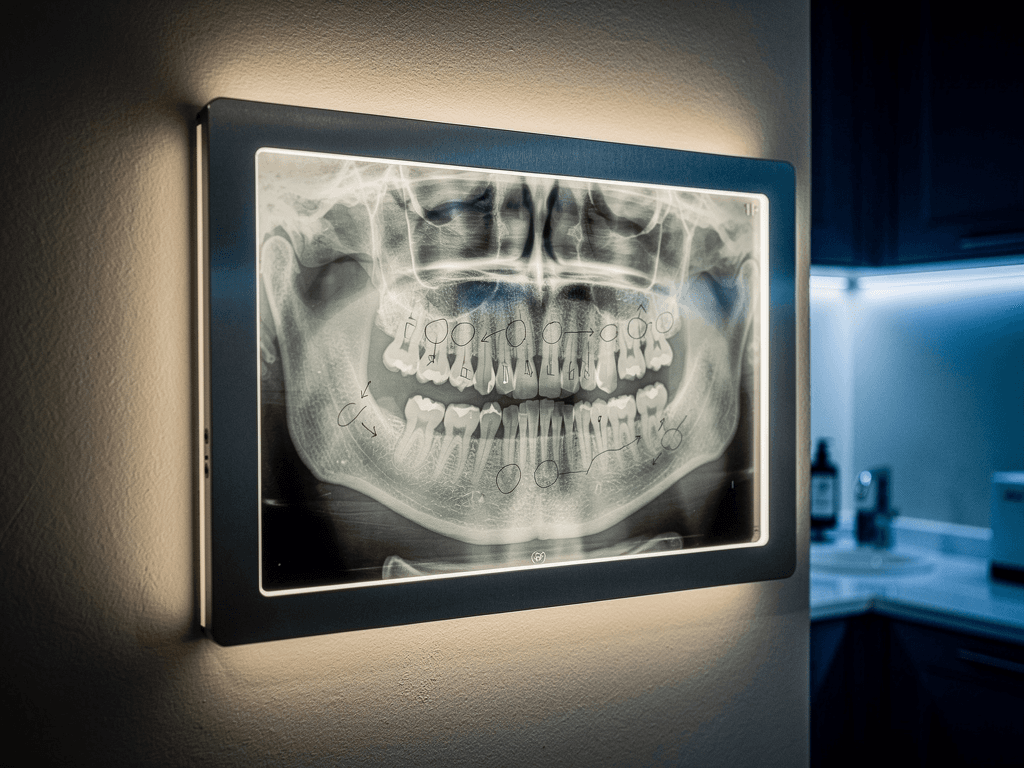
3. Reading radiographs alongside the clinician
The use case the dental press writes about. AI image-analysis tools (Pearl, Overjet, Diagnocat are the names that come up most often in UK practices) ingest bitewings, periapicals, and panoramics, then mark up suspected caries, periapical lesions, bone loss, and root fractures.
The clinician still reads the radiograph. The AI is a second pair of eyes.
Rough setup: £150 to £400 per chair per month.
Rough return at 90 days: not about chair-time savings. The return is on treatment-plan acceptance. A patient presented with a marked-up radiograph showing exactly what the clinician is concerned about converts on complex treatment at materially higher rates than one shown a plain image. Principal dentists report this as the biggest case-presentation upgrade in a decade.
The catch: it is the use case with the slowest payback measurement. Treatment plan conversion takes weeks to read. Owners impatient for hard ROI numbers in 30 days often abandon it before the data is in.
4. Writing the patient letters the clinician does not have time to write
The chairside scribe category. Heidi, Dentr, and a handful of smaller UK-based tools listen to the clinical consultation, draft the patient summary, the treatment plan letter, the referral letter, and the follow-up.
The clinician dictates the plan in 90 seconds at the end of the appointment. The tool writes the 800-word patient letter, the GP referral, and the dental note in 30 seconds.
Rough setup: £80 to £200 per clinician per month.
Rough return at 90 days: 45 minutes per day per principal dentist returned to clinical time or to the family. Across a clinical year, 150 hours plus.
The catch: it works only if the clinician actually dictates. Practices with consistent dictation culture get the value. Practices where the principal jots notes between patients do not.

5. Predicting and preventing no-shows
The newest cluster of tools. Practice management add-ons that score each upcoming appointment by no-show risk based on past behaviour (how often the patient has cancelled, how late they pay, how recently they last attended) and trigger pre-emptive confirmation outreach for high-risk slots.
The medium-risk patient gets a friendly reminder 48 hours out. The high-risk patient gets a polite confirmation call 24 hours out. The low-risk patient gets a standard 24-hour text.
Rough setup: £120 to £300 per month or bundled into a wider recall system.
Rough return at 90 days: UK private no-show rates of 8% to 12% typically drop to 4% to 6%. At an average chair-hour value of £180 to £260 at a private practice, the recovered chair time pays back the tool inside the first fortnight.
6. Drafting marketing copy and patient communication
The least visible use case. The one almost every practice manager already uses, even if they have not told anyone.
Practice teams now use AI writers (Claude, ChatGPT, Jasper) to draft monthly newsletters, social posts, Google Business updates, in-practice signage copy, and patient handouts. What used to take the manager an hour now takes ten minutes plus a review.
Rough setup: £0 to £20 per month per team member.
Rough return at 90 days: four hours per week of practice manager time returned to higher-value work. Almost no risk if the manager reviews everything before it goes out.
The mistake some practices make: letting the AI publish unedited. Patients notice. The voice goes flat. Always review.
What ties these six together
No clinical robotics. No workflow rewrite. No full replacement for staff. They are coverage layers that catch what your team cannot catch when the practice is busy.
The 78% of private practices already using AI use it like this. Quiet, operational, measurable. The marketing pages talk about robots. The practices buying the tools talk about Saturday morning recall lists and the call they missed at 4.47 pm last Tuesday.
Start with the one that maps to your biggest leak this month. If that leak is the phone, the maths is in what a missed call costs a private dental practice.
How to pick which one to try first
The six above are not equal in payback speed. Ranked by how quickly the practice will know if it works:
- Front-desk call handling: 14 days. The missed-call rate and the new-patient booking count move inside two weeks of going live. The fastest read.
- No-show prediction: 30 days. The no-show rate is a clean weekly metric and the chair-hour value is easy to attribute.
- Automated recall and reactivation: 60 days. The first reactivation wave lands in week three; the second-touch sequence completes by day 60.
- Marketing copy drafting: 60 days. Time-saving is felt almost immediately; quality drift is the thing to monitor.
- Treatment-plan drafting and patient letters: 90 days. Workflow change takes a fortnight; consistent dictation habit takes another month.
- Radiograph reading: 120 days. Treatment-plan conversion is a noisy metric that needs volume to read.
A practice with cash to invest in only one tool this year should start with the use case at the top of the list. Speed of feedback compounds. A tool you can measure in 14 days teaches you more about your practice in a month than three tools you cannot measure in 90.
What every one of the six requires from the practice
No tool runs itself. Every use case above requires one named owner inside the practice. For radiograph reading, the principal dentist. For recall, the practice manager. For front-desk cover, the practice manager. For chairside scribe, the clinician using it. For no-show prediction, the practice manager. For marketing copy, whoever writes the newsletter today.
Without a named owner the tool drifts. The owner does not have to be a digital native. They do have to look at the weekly report for ten minutes and either say "this is working" or "this is not." That ten-minute habit is the difference between a tool that stays and a tool that gets cancelled at month four.