AI dental x-ray reading is the use case the dental press gets most excited about, and for once the excitement is mostly earned. In a UK private practice, software that reads a radiograph alongside the clinician is the purest clinical use of AI in dentistry, and it is genuinely useful.
It is also, quietly, the slowest of the common AI use cases to pay back. That is not a reason to avoid it. It is a reason to understand it before you spend, and to know where it sits against the front-desk tools that return money in a fortnight rather than a quarter.
This is the honest owner's guide. What it does, the three names you will hear, what it costs, and where the fastest return actually lives.
What AI dental x-ray reading actually does
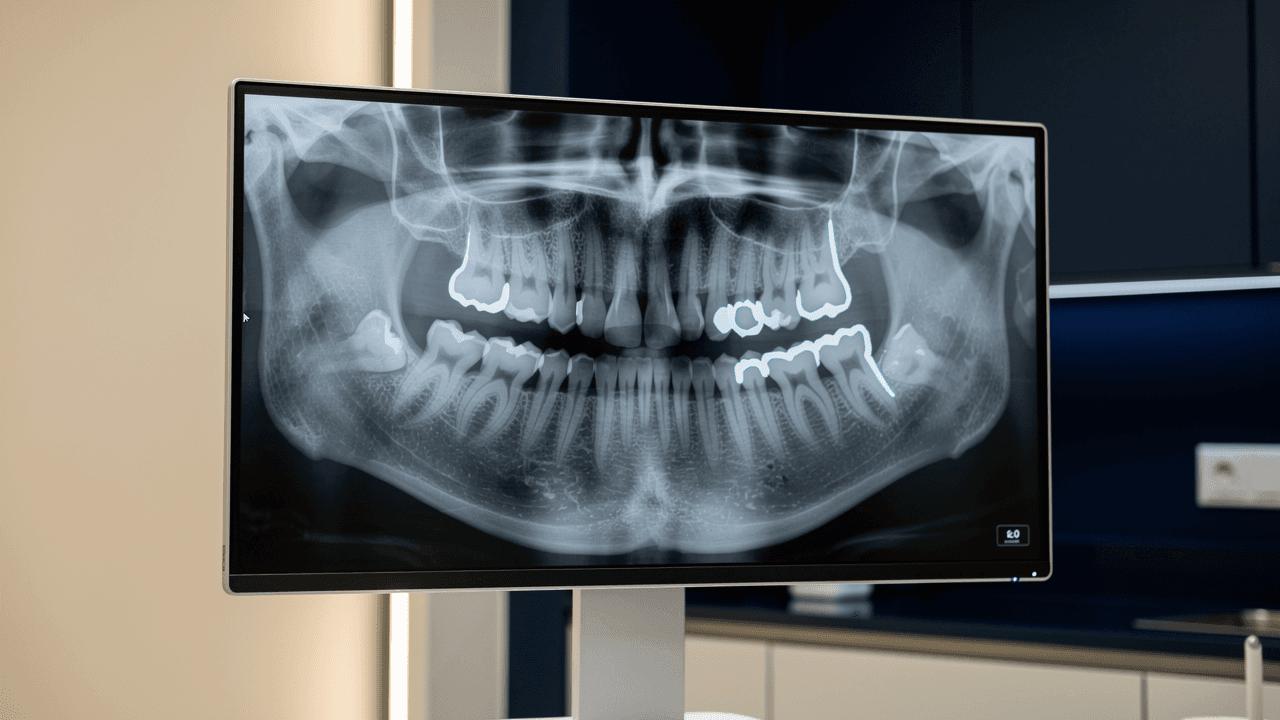
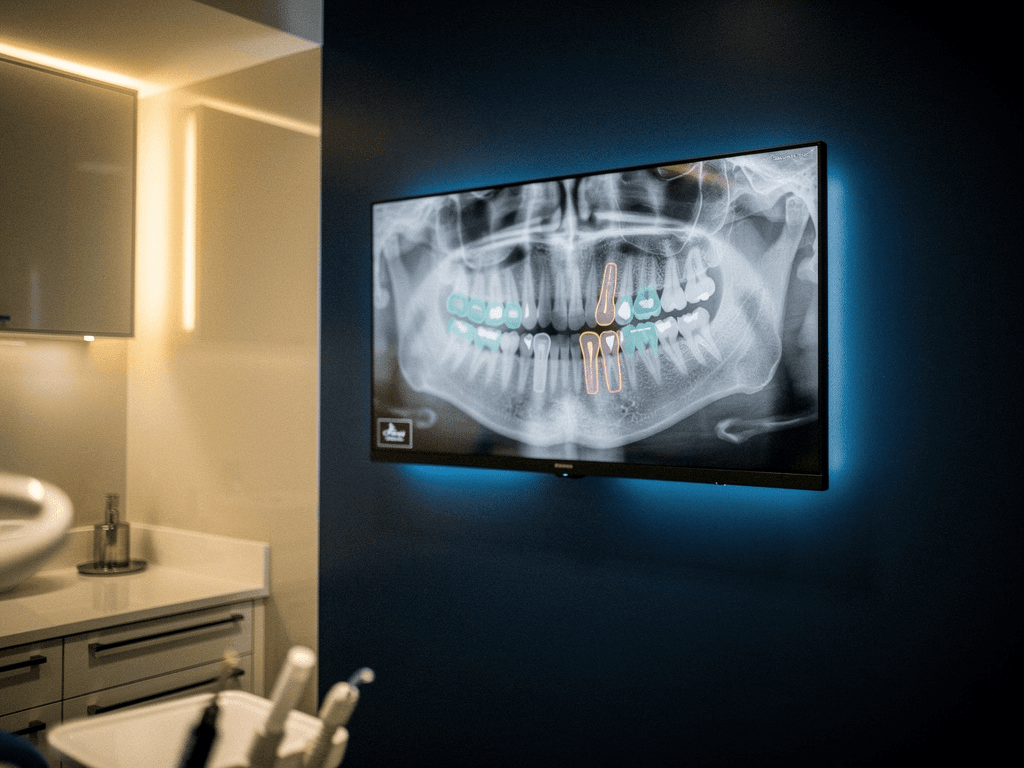
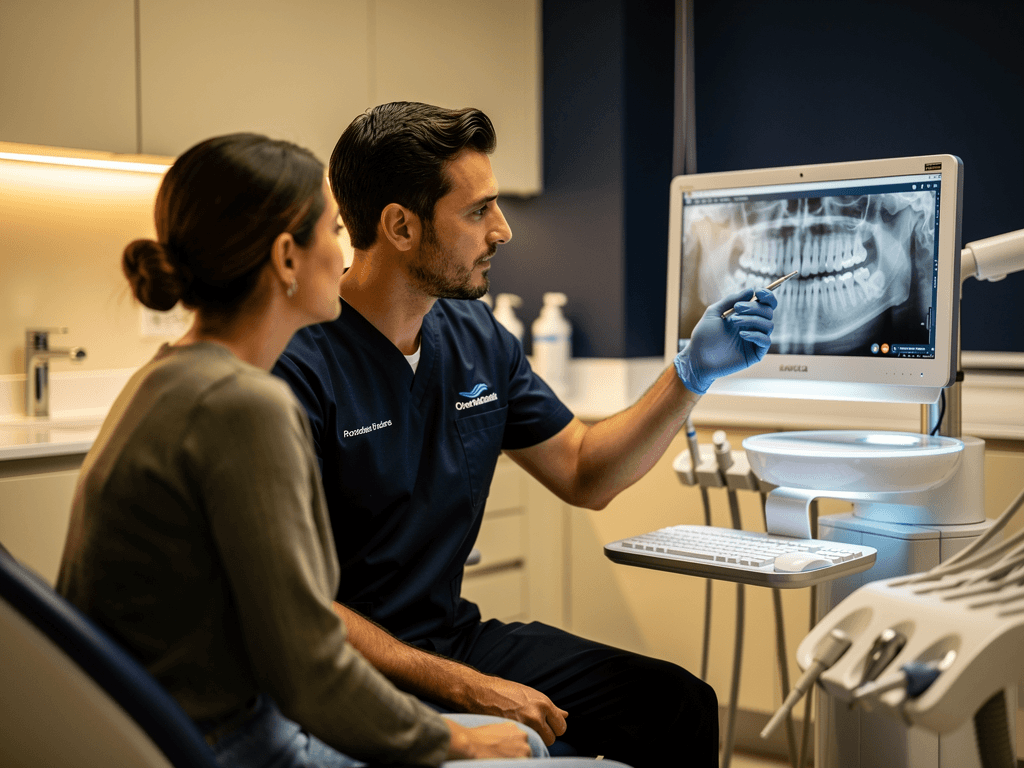
Strip away the marketing and the function is straightforward. The software ingests a digital radiograph, a bitewing, a periapical, or a panoramic, and marks up areas that look like caries, bone loss, periapical lesions, or other findings. It puts a coloured outline and a confidence note on the image, drawing the clinician's eye to things worth a second look.
The crucial word is alongside. The clinician still reads the radiograph and still makes every clinical decision. The software is a second pair of eyes, not a replacement for the first pair. No diagnosis is made by the software on its own. No clinical call is taken out of the dentist's hands. No shortcut is offered around a proper read.
Used well, it does two things. It catches the thing a tired clinician at the end of a long list might glance past. And, because it shows the patient a clearly marked-up image rather than a grey blur, it makes the conversation about treatment far easier to have. That second effect is where most of the practical value turns out to live.
The three names UK practices come across
Three products come up again and again in UK practices, and they are not identical.
Pearl is the most widely known, with regulatory clearance in multiple markets. Its strength is chairside detection: marking up the radiograph in the moment so the clinician and patient can look at it together. It leans into the case-presentation use.
Overjet is strong on analytics and quantification, putting numbers on findings such as bone-loss measurement. It tends to appeal to practices and groups that want to standardise how findings are assessed across clinicians.
Diagnocat has a particular strength in panoramic and 3D, including CBCT analysis, which makes it interesting to practices doing more implant and complex work.
What unites them is the regulatory floor. Serious clinical radiograph tools carry FDA clearance or CE marking, and you should treat that as a baseline requirement, not a bonus. Anything reading clinical images without it does not belong near a patient. Which of the three fits depends on your case mix, not on which has the glossiest website. For where this sits among the other things practices are doing, see how private dental practices use AI in 2026.
What it costs and what it returns
Pricing is usually per chair per month, broadly £150 to £400 depending on the product and the size of the practice. For a multi-chair practice that adds up, so the return has to be real.
Here is the part owners get wrong. The return on clinical radiograph software is not chair time, and it is not really about catching pathology a good clinician would miss, valuable as that is for care. The measurable return is treatment-plan acceptance.
A patient who is told they need treatment hears an opinion. A patient who is shown their own radiograph with the problem clearly outlined sees a reason. The second patient accepts complex treatment more readily, because the marked-up image does the persuading that a verbal explanation cannot. In a private practice where a single implant or larger restorative plan is worth thousands, a modest lift in acceptance across the year is where the software pays for itself. The mechanics of why high-value treatment conversations succeed or leak are covered in where high-value treatment enquiries leak.
Put rough numbers on it. A practice presenting two or three larger restorative or implant plans a week, where a single accepted case is worth several thousand pounds, needs only a handful of extra yeses across a year to cover the per-chair fee many times over. The software does not create the demand. It makes the case the patient was already half-considering far easier to accept, because they can see the problem instead of being asked to take it on trust.
That is the real business case. Not fewer missed lesions, though that matters clinically. Better-understood treatment plans that patients say yes to.
Why it has the slowest payback to measure
This is the honest caveat no clinical-AI vendor leads with. Treatment-plan acceptance is a slow, noisy thing to measure.
You cannot read it in a week. Acceptance varies by patient, by treatment type, by clinician, and by how the conversation is handled, so it takes weeks of consistent use and a decent volume of cases before a trend separates from the noise. Realistically you are looking at something like a 120-day window before the numbers tell you anything trustworthy.
Owners who expect a 30-day return get impatient, conclude it is not working, and drop it right before the data would have shown the lift. The tool did not fail. The measurement horizon was wrong from the start. If you buy clinical radiograph software, buy it knowing you are committing a quarter before you judge it, and make sure your clinicians actually use it consistently in that window, because patchy use produces patchy data and a false negative.
What you need in place before you buy
Three things have to be true before clinical radiograph software earns its keep.
Digital radiography. The software reads digital images. If any part of your imaging is still analogue, sort that first.
A named clinical owner. Someone, usually the principal, has to own the habit of using the markup in the case conversation. Software bought and then half-used returns nothing. This is a behaviour change as much as a purchase.
A consistent case-presentation routine. The value comes from showing patients their marked-up images as a normal part of the treatment discussion. If your practice does not present cases consistently today, the software amplifies a habit you do not yet have. Build the habit, then the tool makes it sharper.
If those three are not in place, the money is better spent elsewhere until they are. Adoption across UK dentistry is already high, with around 78% of practices using at least one AI tool per the BDA's 2025 survey, but high adoption is not the same as high return. The return depends on the three conditions above.
Where the fastest-ROI AI actually sits
Here is the part a vendor in the radiograph business would never tell you, which is exactly why it is worth saying.
Clinical x-ray reading is the highest-prestige AI use case and the slowest to pay back. The fastest-paying AI in a dental practice is not clinical at all. It is the front desk. An AI receptionist that answers the calls a busy practice misses, qualifies the enquiry, and books straight into the diary shows a measurable return inside about 14 days, because a recovered new-patient call is money you can count almost immediately, against a roughly 120-day horizon for treatment-plan acceptance.
So if you are deciding where to start with AI and you want the return that funds everything else, start where the feedback is fastest: the phone. Then, with that paying for itself, move to the clinical tools whose return is real but patient. This is not a reason to skip radiograph software. It is the right order to buy in. For the full decision on where to begin before the 2027 adoption curve steepens, see where UK dental practices should start with AI before 2027.
AI dental x-ray reading deserves its reputation as the most impressive clinical tool in the room. Just go in clear-eyed: name a clinical owner, commit a quarter to measuring acceptance, and start with the front-desk return that pays for the rest. Do it in that order and both halves earn their keep.